A Knee Replacement That Costs $9,000 in China Can Become $95,000 in the U.S. — and Insurers May Just Shrug
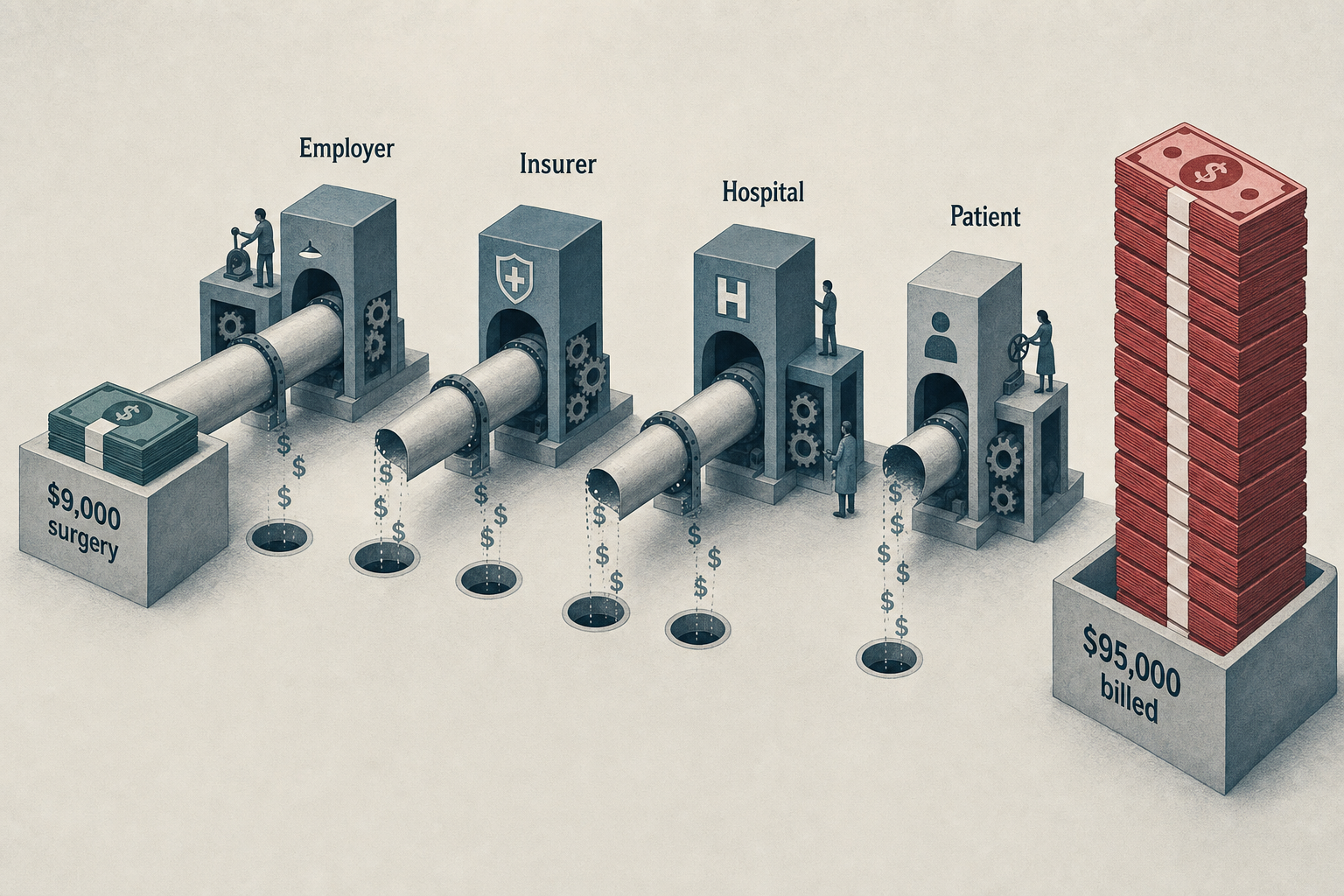
$9,000 is a reasonable all-in price for a knee replacement at a JCI-accredited hospital in China. In the United States, the same episode typically runs from about $30,000 to $68,000 by common commercial benchmarks; once facility fees, anesthesia, imaging, implants, and post-acute care are layered in, the high end of the bill can approach $95,000
$9,000 is a reasonable all-in price for a knee replacement at a JCI-accredited hospital in China. In the United States, the same episode typically runs from about $30,000 to $68,000 by common commercial benchmarks; once facility fees, anesthesia, imaging, implants, and post-acute care are layered in, the high end of the bill can approach $95,000 [1][2].
The same joint. The same class of titanium-and-polyethylene prosthesis. The same surgical playbook. Often, even the same training lineage: many orthopedic surgeons at internationally accredited hospitals in China trained or completed fellowships in the United States, Europe, or Singapore.
So why, if the same operation can be safely delivered abroad for $9,000 and domestically costs $68,000 — or even $95,000 — doesn’t the U.S. market arbitrage the gap?
Because the payer who could fix it usually does not capture the savings.
The gap is not hidden. It persists because the U.S. system is designed so that eye-watering prices can endure as long as the people making the purchasing decisions do not bear the consequences.

The gap has little to do with quality
The lazy answer is that U.S. care is expensive because U.S. care is better. Sometimes that is true. Usually, it is not.
Joint replacement is not experimental oncology. It is a mature, standardized, high-volume procedure. The ingredients are familiar: pre-op imaging, anesthesia, a prosthesis, an operating room, antibiotics, physical therapy, follow-up. A good knee replacement depends on surgeon volume, infection control, implant quality, rehabilitation, and patient selection. It does not require a $70,000 price tag to exist.
Joint Commission International, or JCI, accredits hospitals outside the United States on dimensions such as patient safety, infection prevention, medication management, and surgical processes [3]. Accreditation is not magic, but it is a real filter. It separates hospitals built for global patients from the vague category of “medical tourism,” which includes both elite centers and risky discount clinics.
The implant argument is not as strong as Americans often assume, either. Major global implant manufacturers sell into Asia, Europe, and the Middle East. A knee prosthesis used in Shanghai is not automatically a cheap counterfeit. In higher-end hospitals, the brand, model, and country of origin are documented and available on request.
The United Kingdom is a particularly useful comparison because it cuts around the objection that China is cheaper simply because labor is cheaper. Private knee replacement in the UK runs about $12,700 to $19,000 [1]. That is the market price in a developed country’s private system. The U.S. remains far above it.
And this is not just about knees. In the U.S., a CT or MRI scan costs roughly $400 to $7,000 depending on the body part, while in China it costs $42 to $280. Routine lab work — a complete blood count, a basic metabolic panel — runs $25 to $125 in the U.S. and $14 to $70 in China [1]. These are not exotic procedures. They are the plumbing of the health system.
 The broader research literature says the same thing. One JAMA study found that hospital-administered drugs in the U.S. were priced at about 250% of the average in 11 comparable countries [4]. Health policy researchers keep arriving at the same conclusion: the U.S. does not spend too much because patients consume dramatically more care. It spends too much because prices are higher [5].
That distinction matters. If Americans were getting knee replacements and MRIs at twice the rate of everyone else, the policy answer would be utilization control. If the same services cost three times, five times, or ten times as much, the answer is price discipline. The U.S. has chosen not to do that.
The broader research literature says the same thing. One JAMA study found that hospital-administered drugs in the U.S. were priced at about 250% of the average in 11 comparable countries [4]. Health policy researchers keep arriving at the same conclusion: the U.S. does not spend too much because patients consume dramatically more care. It spends too much because prices are higher [5].
That distinction matters. If Americans were getting knee replacements and MRIs at twice the rate of everyone else, the policy answer would be utilization control. If the same services cost three times, five times, or ten times as much, the answer is price discipline. The U.S. has chosen not to do that.
Why insurers do not fix it
The most common response from patients is moral outrage: “Why doesn’t my insurer just send people abroad and split the savings?”
Because commercial insurance is not a clean market transaction. It is a chain of partial incentives.
Roughly two-thirds of covered workers are in self-funded plans, meaning the employer — not the carrier — is on the hook for the claims [6]. That should make employers eager to pursue cross-border savings. Some self-insured groups and health-sharing organizations have indeed built pathways for elective procedures overseas, sometimes including airfare and cost-sharing [7][8]. But these are exceptions.
Three things explain why, by default, almost no one moves.
First, building an overseas network is administratively annoying. Credentialing, outcomes reporting, bundled-price negotiation, medical-record handoffs, complication management, compliant consent frameworks. Those costs are modest relative to the $50,000 saved on a single surgery, but they are not trivial when spread across a population in which only a small fraction of members will need the procedure each year.
Second, mandatory offshore routing is legally fraught. Employers can design incentives, but “fly to China for your knee or pay an extra $50,000” is not language most benefits lawyers want in a plan document. Under ERISA, employers have room — and obligations.
Third, and most underestimated, is churn. Employees change jobs. Employers change carriers. Commercial plans often model member tenure at 18 to 24 months [10]; the median tenure for U.S. private-sector workers in 2024 was 3.7 years [11]. Suppose a 58-year-old employee needs surgery. Domestic episode: $68,000. Cross-border bundled episode: $9,000 surgery plus $4,000 in travel and coordination. Gross savings: $55,000. But this year’s savings accrue to the employer; next year, the patient may have moved on; and the long-term gains — better mobility, fewer opioid prescriptions, delayed disability — land with the next employer, the next insurer, Medicare, or no one at all.
That is a time-horizon externality. The party with the power to build the cheaper pathway may not still be around when the benefits arrive.
So the plan does what U.S. health care usually does: it negotiates a “discount” off an inflated charge, calls it savings, and moves on.

What would actually move the needle
The fix is not mysterious. It is just uncomfortable. Reference pricing. The payer sets a ceiling price for a procedure. Patients who choose a hospital above the ceiling pay the difference. A California public purchaser set a $30,000 cap on joint replacement, and spending fell while previously high-priced hospitals cut prices rather than lose volume [12]. Medicare’s bundled-payment experiments for joint replacement reduced episode payments without worsening measurable quality metrics [13]. When the reference price is not “the cheaper hospital down the road” but “the global fair price,” the tool becomes sharper. Direct contracting. Large self-insured employers can contract directly with centers of excellence — domestic or international — using bundled prices and transparent outcomes data. Some already do this for spine, joints, bariatrics, and transplant [7]. Value-based benefit design with real patient incentives. If a patient helps the plan avoid $60,000 in excess spending, that patient should get more than a $25 gift card. Waive the deductible. Cover travel. Pay for a companion. Share the savings with the person who actually has to go under anesthesia, to a level that makes choosing the better route rational. Transparency with teeth. Publishing prices is useful. But transparency without purchasing discipline is a museum exhibit — everyone can look, and no one acts.
The spread is the design
Patients did not create a system where a scan costs $280 in one country and $7,000 in another. They did not write hospital chargemasters, negotiate network contracts, or define prudence as extracting a discount from a fictional price. The spread persists not because patients are ignorant. It persists because the system paying the bill has no durable financial incentive to close it. The $86,000 difference between a $9,000 operation and a $95,000 episode is not market failure. It is the market working exactly as designed — for the people who actually have a voice in pricing decisions.
This article was originally published on the author’s personal website and republished on Medium with permission. About the author: Reed focuses on the economics of cross-border care that do not add up, and on the data patients and payers actually need to make decisions. More analysis at medicaltochina.com.
References
[1] 2023–2024 international health care cost references, citing the International Federation of Health Plans (iFHP) and MedBridge-style private-market benchmarks. Ranges used: China JCI knee replacement $4,200–$14,000; UK private $12,700–$19,000; U.S. $30,000–$68,000; China CT/MRI $42–$280; U.S. CT/MRI $400–$7,000; China routine labs $14–$70; U.S. $25–$125. https://www.ifhp.com/price-report/ [2] Blue Cross Blue Shield Association, "A Study of Cost Variations for Knee and Hip Replacement Surgeries in the U.S." https://www.bcbs.com/the-health-of-america/reports/study-of-cost-variations-knee-and-hip-replacement-surgeries-us [3] Joint Commission International, accreditation overview. https://www.jointcommissioninternational.org/what-we-offer/accreditation/ [4] A. W. Mulcahy et al., "International Prescription Drug Price Comparisons," RAND, 2021; and similar JAMA analyses of hospital-administered drug prices. https://www.rand.org/pubs/research_reports/RR2956.html [5] I. Papanicolas, L. R. Woskie, A. K. Jha, "Health Care Spending in the United States and Other High-Income Countries," JAMA, 2018. https://jamanetwork.com/journals/jama/fullarticle/2674671 [6] KFF, "2023 Employer Health Benefits Survey," self-funded plans section. https://www.kff.org/report-section/ehbs-2023-section-10-plan-funding/ [7] NFL Player Care Foundation / NFL Joint Replacement Program. https://www.nflplayercare.com/ [8] Samaritan Ministries membership-sharing model. https://samaritanministries.org/ [9] CMS, Medical Loss Ratio rules. https://www.cms.gov/marketplace/private-health-insurance/medical-loss-ratio [10] Health Affairs research on insurance churn and coverage instability. https://www.healthaffairs.org/doi/10.1377/hlthaff.2016.0455 [11] U.S. Bureau of Labor Statistics, Employee Tenure Summary, 2024. https://www.bls.gov/news.release/tenure.nr0.htm [12] J. C. Robinson, T. T. Brown, "Increases In Consumer Cost Sharing Redirect Patient Volumes And Reduce Hospital Prices For Orthopedic Surgery," Health Affairs, 2013. https://www.healthaffairs.org/doi/10.1377/hlthaff.2012.1198 [13] CMS Innovation Center, Bundled Payments for Care Improvement evaluation reports. https://innovation.cms.gov/innovation-models/bundled-payments
Ready to start your health journey?
Our medical concierge team is available around the clock to answer your questions and help plan your treatment.

